Infectious Diseases Weekly Report (IDWR)
速報データ 2013年第10週(3月04日ー3月10日)
http://www.nih.go.jp/niid/ja/data/3334-idwr-sokuho-data-j-1310.html
定点把握疾患(週報告)、報告数、定点当り報告数、都道府県別
http://www.nih.go.jp/niid/images/idwr/sokuho/idwr-2013/201310/2013-10-teiten.pdf
報告数·定点当り報告数、疾病·都道府県別
2013年第10週(3月04日ー3月10日)
インフルエンザ
都道府県、定点当り, 週当りの報告数、
愛知県 27'27 5'317件
福井県 21'38 684件
鹿児島県 21'09 1'961件
徳島県 20'97 797件
広島県 20'66 2'376件
岐阜県 19'97 1'737件
高知県 19'77 949件
山口県 19'09 1'317件
次回の2013年第11週(3月11日ー3月17日)の更新は2013年3月26日です
定点把握疾患(週報告)、累積報告数、累積定点当り報告数、都道府県別
http://www.nih.go.jp/niid/images/idwr/sokuho/idwr-2013/201310/2013-10-teiten-ruiseki.pdf
累積報告数、累積定点当り報告数、疾病·都道府県別
2013年第10週(3月04日ー3月10日)
インフルエンザ
都道府県·累積定点当り報告数· 累積報告数
愛知県 297'76 57'765件
鹿児島県 240'05 22'325件
新潟県 237'76 22'587件
広島県 233'57 26'861件
愛媛県 233´52 14'245件
長野県 222'85 19'388件
福岡県 221'43 43'844件
千葉県 219'18 45'908件
宮崎県 214'51 12'656件
静岡県 209'55 29'128件
岐阜県 209'39 18'217件
埼玉県 207'12 49'916件
沖縄県 204'47 11'959件
茨城県 202'54 24'305件
疾病毎定点当り報告数(過去10年間との比較) 2003年ー2013年
http://www.nih.go.jp/niid/images/idwr/sokuho/idwr-2013/201310/binder10.pdf
疾病毎定点当り報告数(過去10年間との比較) 2003年ー2013年
インフルエンザ(風邪)の各週の発生率, 2003年ー2013年
2013年第4週1月20日ー1月26日と2013年第5週1月20日ー1月26日がインフルエンザ(風邪)の発生率が頂点·最高に達した。
注目すべき感染症
http://www.nih.go.jp/niid/ja/chumoku.html
Infectious Diseases Weekly Report 2012年第50週12月10日ー12月16日
2012年12月28日 発行
インフルエンザ(風邪)
http://www.nih.go.jp/niid/ja/flu-m/flu-idwrc/3055-idwrc-1250.html
| |||||||||||||
2012年12月21日 発行
インフルエンザ(風邪)
http://www.nih.go.jp/niid/ja/flu-m/flu-idwrc/3023-idwrc-1249.html
| ◆ インフルエンザ インフルエンザ(Influenza)は、インフルエンザウイルスを病原体とする急性の呼吸器感染症で、毎年世界中で流行がみられている。典型的な発症例では1~4日間の潜伏期間を経て、突然に発熱(38℃以上の高熱)、頭痛、全身倦怠感、筋肉痛・関節痛などが出現し、鼻水・咳などの呼吸器症状がこれに続く。通常は1週間前後の経過で軽快するが、いわゆる「かぜ」と比べて全身症状が強いのが特徴である。主な感染経路はくしゃみ、咳、会話等で口から発する飛沫による飛沫感染であり、他に接触感染もあるといわれている(CDCホームページ:http://www.cdc.gov/flu/professionals/infectioncontrol/healthcaresettings.htm>)。 インフルエンザを予防する手段としては、まずはワクチンの接種があげられる。また、感染対策としては、飛沫感染対策としての咳エチケット、接触感染対策としての手洗い等の手指衛生が重要である。インフルエンザでは、たとえ感染者であっても、全く症状のない不顕性感染例や、感冒様症状のみでインフルエンザウイルスに感染していることを本人も周囲も気が付かない軽症例も少なくないため、特にヒト-ヒト間の距離が短く、濃厚な接触機会の多い学校、幼稚園、保育園等の小児の集団生活施設においては可能である場合は職員も含めて全員が咳エチケット、手指衛生を実行するべきである(厚生労働省インフルエンザQ&A:http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou01/qa.html)。 感染症発生動向調査では、感染性胃腸炎は全国約3,000カ所の小児科定点からの報告に基づいている。感染性胃腸炎の定点当たり報告数は2012年第42週以降増加が続いており、第48週の定点当たり報告数は18.00(報告数56,677)となった。2002年以降の過去10年の同時期と比較した場合、2006年(定点当たり報告数21.86)に次ぐ高い値である(図1)。都道府県別では鹿児島県(37.42)、宮崎県(34.72)、福井県(33.59)、大分県(28.67)、富山県(28.03)、愛媛県(26.00)、熊本県(24.94)の順となっており、大阪府を除く46都道府県で前週の報告数を上回った(図2)。2012年第36~48週の定点当たり累積報告数は83.59(累積報告数263,344)であり、年齢群別割合では0~1歳24.9%、2~3歳21.0%、4~5歳17.3%、6~7歳10.1%の順となっている。 感染症発生動向調査では、全国約5,000カ所(小児科定点約3,000、内科定点約2,000)のインフルエンザ定点からの報告に基づいてインフルエンザの発生動向を分析している。インフルエンザの定点当たり報告数は、2012年第43週以降増加が続いており、第49週の定点当たり報告数0.57(報告数2,832)は、前週(0.31)と比較してほぼ倍増した(図1)。都道府県別では佐賀県(5.58)、沖縄県(2.81)、群馬県(2.66)、千葉県(1.26)、岐阜県(1.05)、大分県(1.05)、埼玉県(1.04)、山梨県(1.00)の順となっており、37都道府県で前週よりも増加が認められた(図2)。 2012年第36~49週に国内では170検体のインフルエンザウイルスの検出が報告されており、AH1pdm09が15件(8.8%)、AH3亜型(A香港型)141件(82.9%)、B型14件(8.2%)とこれまでのところAH3亜型が大半を占めている(図3)。
今シーズン(2012/2013年シーズン)のインフルエンザの定点当たり報告数は今後さらに増加し、まもなく全国的な流行開始の指標である1.00を上回る可能性が高いと予想される。インフルエンザの予防の基本はインフルエンザワクチンの接種であり、ワクチンの接種を必要としながらも、現時点ではまだ接種が実施されていない場合は速やかに接種することが望まれる。今後ともインフルエンザの発生動向には注意深い観察が必要である。 |

感染症流行予測調査
National Epidemiological Surveillance of Vaccine Preventable Diseases
http://www.nih.go.jp/niid/ja/yosoku-index.html
2013年1月21日発表
インフルエンザ抗体保有状況
2012年度速報第3号
http://www.nih.go.jp/niid/ja/flu-m/253-idsc/yosoku/sokuhou/3118-flu-yosoku-rapid2012-3.html
| インフルエンザ抗体保有状況 -2012年速報第3報- (2013年1月21日現在) | |
| はじめに 感染症流行予測調査事業における「インフルエンザ感受性調査」は,毎年,インフルエンザの本格的な流行が始まる前に,インフルエンザに対する国民の抗体保有状況(免疫状況)を把握し,抗体保有率が低い年齢層に対するワクチン接種の注意喚起ならびに今後のインフルエンザ対策における資料とすることを目的として実施している。 現在使われているインフルエンザワクチンは,A(H1N1)亜型,A(H3N2)亜型,B型(ビクトリア系統あるいは山形系統)の3つのインフルエンザウイルスがワクチン株として用いられているが,インフルエンザ感受性調査では,これら3つのワクチン株に加え,ワクチンに用いられなかった別系統のB型インフルエンザウイルスについて抗体保有状況の検討を行っている。 本速報では,2012年度の調査によるインフルエンザに対する年齢群別抗体保有状況および前年度調査との比較について掲載する。 | |
| 1. 調査対象および方法 2012年度の調査は,25都道府県から各198名,合計4,950名を対象として実施された。 インフルエンザウイルスに対する抗体の有無および抗体価の測定は,対象者から採取された血液(血清)を用いて,調査を担当した都道府県衛生研究所において赤血球凝集抑制試験(HI法)により実施された。採血時期は原則として2012年7~9月(例年のインフルエンザの流行シーズン前かつワクチン接種前)とした。また,HI法に用いたインフルエンザウイルス(調査株)は以下の4つであり,このうちa)~c)は2012/13シーズンのインフルエンザワクチンに用いられているウイルス,d)はワクチン株とは異なる系統のB型インフルエンザウイルスであるが,抗体保有状況の把握が必要と考えられるウイルスである。 a) A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型] b) A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型] c) B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)] d) B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)] | |
| 2. 調査結果 2013年1月21日現在,北海道,山形県,福島県,茨城県,栃木県,群馬県,千葉県,東京都,神奈川県,新潟県,富山県,石川県,福井県,山梨県,長野県,静岡県,愛知県,三重県,京都府,山口県,愛媛県,高知県,佐賀県,熊本県,宮崎県の25都道府県から合計6,794名の対象者についての結果が報告された。5歳ごとの年齢群別対象者数は,0-4歳群:857名,5-9歳群:538名,10-14歳群:605名,15-19歳群:540名,20-24歳群:534名,25-29歳群:592名,30-34歳群:521名,35-39歳群:531名,40-44歳群:492名,45-49歳群:385名,50-54歳群:372名,55-59歳群:316名,60-64歳群:284名,65-69歳群:116名,70歳以上群:111名であった。 なお,本速報における抗体保有率とは,感染リスクを50%に抑える目安と考えられているHI抗体価1:40以上の抗体保有率を示し,抗体保有率が60%以上を「高い」,40%以上60%未満を「比較的高い」,25%以上40%未満を「中程度」,10%以上25%未満を「比較的低い」,5%以上10%未満を「低い」,5%未満を「きわめて低い」と表す。 | |
| 1)年齢群別抗体保有状況 A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型]:図1上段 本ウイルスは2009年に世界的大流行(パンデミック)を起こしたインフルエンザウイルスである。2009/10シーズンは本ウイルスを用いた単価ワクチンが製造され,従来のインフルエンザワクチン(3価ワクチン)とは別に接種が行われたが,2010/11シーズン以降は3シーズン続けてワクチン株の1つとして選定されている。 本ウイルスに対する抗体保有率は,0-4歳群および55歳以上の各年齢群で中程度以下の抗体保有率(22~36%)であったが,それ以外の年齢群は比較的高い~高い抗体保有率(43~80%)であった。中でも10~24歳の各年齢群は60%以上の抗体保有率であり,15-19歳群で最も高かった。全体の抗体保有率は51%であり,調査株中最も高かった。 A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型]:図1下段 本ウイルスは2012/13シーズンのワクチン株の1つとして選定されたウイルスであり,2010/11~2011/12シーズンにワクチン株であったA/Victoria(ビクトリア)/210/2009から変更となった。 本ウイルスに対する全体の抗体保有率は調査株中2番目に低い40%であった。年齢群別では5~44歳の各年齢群および70歳以上群は比較的高い抗体保有率(40~54%)であったが,それ以外の年齢群は中程度以下の抗体保有率(22~34%)であり,特に0-4歳群は25%未満の抗体保有率であった。 B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)]:図2上段 本ウイルスは2010年に分離されたB型インフルエンザウイルスであり,2012/13シーズンは4シーズンぶりに山形系統の本ウイルスがワクチン株の1つに選定された。 本ウイルスに対する抗体保有率は,全体では31%と調査株中最も低く,年齢群別では20-24歳群をピークに15~29歳の各年齢群のみが40%以上の抗体保有率(48~65%)であった。それ以外の年齢群は中程度以下の抗体保有率(9~37%)を示し,中でも10歳未満および50歳以上の各年齢群は25%未満の抗体保有率であった。 B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)]:図2下段 本ウイルスは2009/10~2011/12シーズンまで3シーズン連続してワクチン株に選ばれたウイルスであり,本年度調査におけるビクトリア系統の代表として用いた。 本ウイルスに対する抗体保有率は,0-4歳群および60歳以上の各年齢群で中程度以下の抗体保有率(20~32%)であったが,それ以外の年齢群は比較的高い~高い抗体保有率(41~69%)であった。中でも35~44歳の各年齢群は60%以上の抗体保有率であり,35-39歳群で最も高かった。全体の抗体保有率は調査株中2番目に高い47%であった。 |
図1
 図2  |
| 2)年齢群別抗体保有状況の前年度調査との比較 A(H1N1)pdm09亜型:図3上段 A(H1N1)pdm09亜型については,2009/10~2012/13シーズンのワクチン株(2009/10シーズンは単価ワクチンとして)および2009~2012年度の調査株にA/California(カリフォルニア)/7/2009が連続して用いられた。2009年度は多くの年齢群で10%未満の抗体保有率であり,全体でも8%と低かったが,2010年度にはすべての年齢群で上昇し,全体では40%の抗体保有率であった(グラフなし)。2011年度もすべての年齢群で抗体保有率の上昇がみられ,全体では49%であった。これらの上昇には2009/10および2010/11シーズンにおける流行1),2)が大きく影響していると考えられた。2012年度は多くの年齢群で前年度よりもさらに上昇し,全体の抗体保有率は51%であったが,2011/12シーズンはA(H1N1)pdm09亜型の流行がほとんどみられなかった3)ことを踏まえると,同じワクチン株が連続して用いられたことによる(ワクチン接種者あるいは感染者における)ブースター効果により,調査時まで抗体保有が持続していた影響も考えられた。 A(H3N2)亜型:図3下段 A(H3N2)亜型については,A/Victoria(ビクトリア)/210/2009が2010/11~2011/12シーズンのワクチン株および2010~2011年度調査株に連続して用いられたが,2012/13シーズンのワクチン株および2012年度の調査株はA/Victoria(ビクトリア)/361/2011に変更となった。2010年度は全体で40%の抗体保有率であったが(グラフなし),2011年度には50%に上昇しており,2010/11シーズンにみられたA(H3N2)亜型の流行2)が一因と考えられた。2012年度は調査株の変更により,すべての年齢群で抗体保有率は低下し,全体では40%の抗体保有率であった。 B型(山形系統)]:図4上段 山形系統については,4シーズンぶりにワクチン株の1つに選定され,2012年度の調査株は2012/13シーズンのワクチン株であるB/Wisconsin(ウィスコンシン)/1/2010が用いられた。2011年度にも本ウイルスが調査株として用いられ,抗体保有率はすべての年齢群で40%未満であり,全体では18%程度であった。2012年度はほとんどの年齢群で上昇し,全体では31%の抗体保有率となった。これは2011/12シーズンの中盤以降にみられた山形系統の流行3)が影響の一因として考えられた。 B型(ビクトリア系統):図4下段 ビクトリア系統については,2009/10~2011/12シーズンのワクチン株および2009~2012年度の調査株としてB/Brisbane(ブリスベン)/60/2008が連続して用いられた。全体の抗体保有率は2009年度と2010年度がそれぞれ31%と33%であり(グラフなし),2011年度は45%,2012年度は47%と徐々に上昇していた。これらは2010/11~2011/12シーズンにみられたビクトリア系統の流行2),3)や2011/12シーズンまで3シーズン連続して同じワクチン株が用いられた影響と考えられた。しかし,抗体保有率のピークを示す年齢層がA型や山形系統と異なる傾向については不明である。 |
図3
 図4  |
| コメント 今シーズンは2013年1月10日現在,病原微生物検出情報におけるインフルエンザウイルス分離・検出速報によると,2012年第36週~2013年第2週(9月3日~1月10日)の期間にA(H1)pdm09亜型が25件,A(H3)亜型が411件,B型が41件(山形系統:12件,ビクトリア系統:21件,系統不明:8件)の報告があり,現時点では主にA(H3)亜型が分離・検出されている4)。また,感染症発生動向調査によるインフルエンザ患者の定点あたり報告数は2012年第50週(12月10日~16日)に全国的な流行開始の指標となる1.0を上回り,2013年第2週(1月7日~13日)現在12.07と急増している5)。まだ予防接種を受けていない者,特に本調査において抗体保有率が低かった年齢層においては,ワクチン接種等の早めの予防対策が望まれる。 | |
| 1)インフルエンザ 2009/10シーズン 病原微生物検出情報 月報,Vol.31,No.9:p248-250 2)インフルエンザ 2010/11シーズン 病原微生物検出情報 月報,Vol.32,No.11:p314-316 3)インフルエンザ 2011/12シーズン 病原微生物検出情報 月報,Vol.33,No.11:p285-287 4)インフルエンザウイルス分離・検出速報 2012/13シーズン URL:http://www.nih.go.jp/niid/ja/iasr-inf.html 5)インフルエンザ患者発生状況 URL:http://www.nih.go.jp/niid/images/idsc/disease/influenza/pdm2013-scv/02influenza.csv | |
国立感染症研究所 感染症情報センター/インフルエンザウイルス研究センター | |
2012年12月27日発表
インフルエンザ抗体保有状況
2012年度速報第2号
http://www.nih.go.jp/niid/ja/flu-m/253-idsc/yosoku/sokuhou/3029-flu-yosoku-rapid2012-2.html
| インフルエンザ抗体保有状況 -2012年速報第2報- (2012年12月27日現在) | |
| はじめに 感染症流行予測調査事業における「インフルエンザ感受性調査」は,毎年,インフルエンザの本格的な流行が始まる前に,インフルエンザに対する国民の抗体保有状況(免疫状況)を把握し,抗体保有率が低い年齢層に対するワクチン接種の注意喚起ならびに今後のインフルエンザ対策における資料とすることを目的として実施している。 現在使われているインフルエンザワクチンは,A(H1N1)亜型,A(H3N2)亜型,B型(ビクトリア系統あるいは山形系統)の3つのインフルエンザウイルスがワクチン株として用いられているが,インフルエンザ感受性調査では,これら3つのワクチン株に加え,ワクチンに用いられなかった別系統のB型インフルエンザウイルスについて抗体保有状況の検討を行っている。 本速報では,2012年度の調査によるインフルエンザに対する年齢群別抗体保有状況および前年度調査との比較について掲載する。 | |
| 1. 調査対象および方法 2012年度の調査は,25都道府県から各198名,合計4,950名を対象として実施された。 インフルエンザウイルスに対する抗体の有無および抗体価の測定は,対象者から採取された血液(血清)を用いて,調査を担当した都道府県衛生研究所において赤血球凝集抑制試験(HI法)により実施された。採血時期は原則として2012年7~9月(例年のインフルエンザの流行シーズン前かつワクチン接種前)とした。また,HI法に用いたインフルエンザウイルス(調査株)は以下の4つであり,このうちa)~c)は2012/13シーズンのインフルエンザワクチンに用いられているウイルス,d)はワクチン株とは異なる系統のB型インフルエンザウイルスであるが,抗体保有状況の把握が必要と考えられるウイルスである。 a) A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型] b) A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型] c) B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)] d) B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)] | |
| 2. 調査結果 2012年12月27日現在,北海道,山形県,福島県,茨城県,栃木県,群馬県,千葉県,東京都,神奈川県,新潟県,富山県,石川県,福井県,山梨県,長野県,静岡県,三重県,京都府,山口県,愛媛県,高知県,佐賀県,熊本県,宮崎県の24都道府県から合計6,552名の対象者についての結果が報告された。5歳ごとの年齢群別対象者数は,0-4歳群:828名,5-9歳群:511名,10-14歳群:583名,15-19歳群:514名,20-24歳群:521名,25-29歳群:578名,30-34歳群:507名,35-39歳群:518名,40-44歳群:477名,45-49歳群:370名,50-54歳群:357名,55-59歳群:294名,60-64歳群:272名,65-69歳群:114名,70歳以上群:108名であった。 なお,本速報における抗体保有率とは,感染リスクを50%に抑える目安と考えられているHI抗体価1:40以上の抗体保有率を示し,抗体保有率が60%以上を「高い」,40%以上60%未満を「比較的高い」,25%以上40%未満を「中程度」,10%以上25%未満を「比較的低い」,5%以上10%未満を「低い」,5%未満を「きわめて低い」と表す。 | |
| 1)年齢群別抗体保有状況 A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型]:図1上段 本ウイルスは2009年に世界的大流行(パンデミック)を起こしたインフルエンザウイルスである。2009/10シーズンは本ウイルスを用いた単価ワクチンが製造され,従来のインフルエンザワクチン(3価ワクチン)とは別に接種が行われたが,2010/11シーズン以降は3シーズン続けてワクチン株の1つとして選定されている。 本ウイルスに対する抗体保有率は,0-4歳群および55歳以上の各年齢群で中程度以下の抗体保有率(23~36%)であったが,それ以外の年齢群は比較的高い~高い抗体保有率(43~80%)であった。中でも10~24歳の各年齢群は60%以上の抗体保有率であり,15-19歳群で最も高かった。全体の抗体保有率は51%であり,調査株中最も高かった。 A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型]:図1下段 本ウイルスは2012/13シーズンのワクチン株の1つとして選定されたウイルスであり,2010/11~2011/12シーズンにワクチン株であったA/Victoria(ビクトリア)/210/2009から変更となった。 本ウイルスに対する全体の抗体保有率は調査株中2番目に低い40%であった。年齢群別では5~44歳の各年齢群および70歳以上群は比較的高い抗体保有率(40~54%)であったが,それ以外の年齢群は中程度以下の抗体保有率(22~34%)であり,特に0-4歳群は25%未満の抗体保有率であった。 B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)]:図2上段 本ウイルスは2010年に分離されたB型インフルエンザウイルスであり,2012/13シーズンは4シーズンぶりに山形系統の本ウイルスがワクチン株の1つに選定された。 本ウイルスに対する抗体保有率は,全体では31%と調査株中最も低く,年齢群別では20-24歳群をピークに15~29歳の各年齢群のみが40%以上の抗体保有率(48~65%)であった。それ以外の年齢群は中程度以下の抗体保有率(10~37%)を示し,中でも10歳未満および50歳以上の各年齢群は25%未満の抗体保有率であった。 B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)]:図2下段 本ウイルスは2009/10~2011/12シーズンまで3シーズン連続してワクチン株に選ばれたウイルスであり,本年度調査におけるビクトリア系統の代表として用いた。 本ウイルスに対する抗体保有率は,0-4歳群および60歳以上の各年齢群で中程度以下の抗体保有率(20~33%)であったが,それ以外の年齢群は比較的高い~高い抗体保有率(41~69%)であった。中でも30~44歳の各年齢群は60%以上の抗体保有率であり,35-39歳群で最も高かった。全体の抗体保有率は調査株中2番目に高い47%であった。 |
図1
 図2  |
| 2)年齢群別抗体保有状況の前年度調査との比較 A(H1N1)pdm09亜型:図3上段 A(H1N1)pdm09亜型については,2009/10~2012/13シーズンのワクチン株(2009/10シーズンは単価ワクチンとして)および2009~2012年度の調査株にA/California(カリフォルニア)/7/2009が連続して用いられた。2009年度は多くの年齢群で10%未満の抗体保有率であり,全体でも8%と低かったが,2010年度にはすべての年齢群で上昇し,全体では40%の抗体保有率であった(グラフなし)。2011年度もすべての年齢群で抗体保有率の上昇がみられ,全体では49%であった。これらの上昇には2009/10および2010/11シーズンにおける流行1),2)が大きく影響していると考えられた。2012年度は多くの年齢群で前年度よりもさらに上昇し,全体の抗体保有率は51%であったが,2011/12シーズンはA(H1N1)pdm09亜型の流行がほとんどみられなかった3)ことを踏まえると,同じワクチン株が連続して用いられたことによる(ワクチン接種者あるいは感染者における)ブースター効果により,調査時まで抗体保有が持続していた影響も考えられた。 A(H3N2)亜型:図3下段 A(H3N2)亜型については,A/Victoria(ビクトリア)/210/2009が2010/11~2011/12シーズンのワクチン株および2010~2011年度調査株に連続して用いられたが,2012/13シーズンのワクチン株および2012年度の調査株はA/Victoria(ビクトリア)/361/2011に変更となった。2010年度は全体で40%の抗体保有率であったが(グラフなし),2011年度には50%に上昇しており,2010/11シーズンにみられたA(H3N2)亜型の流行2)が一因と考えられた。2012年度は調査株の変更により,すべての年齢群で抗体保有率は低下し,全体では40%の抗体保有率であった。 B型(山形系統)]:図4上段 山形系統については,4シーズンぶりにワクチン株の1つに選定され,2012年度の調査株は2012/13シーズンのワクチン株であるB/Wisconsin(ウィスコンシン)/1/2010が用いられた。2011年度にも本ウイルスが調査株として用いられ,抗体保有率はすべての年齢群で40%未満であり,全体では18%程度であった。2012年度はほとんどの年齢群で上昇し,全体では31%の抗体保有率となった。これは2011/12シーズンの中盤以降にみられた山形系統の流行3)が影響の一因として考えられた。 B型(ビクトリア系統):図4下段 ビクトリア系統については,2009/10~2011/12シーズンのワクチン株および2009~2012年度の調査株としてB/Brisbane(ブリスベン)/60/2008が連続して用いられた。全体の抗体保有率は2009年度と2010年度がそれぞれ31%と33%であり(グラフなし),2011年度は45%,2012年度は47%と徐々に上昇していた。これらは2010/11~2011/12シーズンにみられたビクトリア系統の流行2),3)や2011/12シーズンまで3シーズン連続して同じワクチン株が用いられた影響と考えられた。しかし,抗体保有率のピークを示す年齢層がA型や山形系統と異なる傾向については不明である。 |
図3
 図4  |
| コメント 今シーズンは2012年12月27日現在,病原微生物検出情報におけるインフルエンザウイルス分離・検出速報によると,2012年第36~51週(9月3日~12月20日)の期間にA(H1)pdm09亜型が15件,A(H3)亜型が177件,B型が26件(山形系統:11件,ビクトリア系統:11件,系統不明:4件)の報告があり,現時点では主にA(H3)亜型が分離・検出されている4)。また,感染症発生動向調査によるインフルエンザ患者の定点あたり報告数は2012年第50週(12月10日~16日)に1.17となり,全国的な流行開始の指標となる1.0を上回った5)。まだ予防接種を受けていない者,特に本調査において抗体保有率が低かった年齢層においては,ワクチン接種等の早めの予防対策が望まれる。 | |
| 1)インフルエンザ 2009/10シーズン 病原微生物検出情報 月報,Vol.31,No.9:p248-250 2)インフルエンザ 2010/11シーズン 病原微生物検出情報 月報,Vol.32,No.11:p314-316 3)インフルエンザ 2011/12シーズン 病原微生物検出情報 月報,Vol.33,No.11:p285-287 4)インフルエンザウイルス分離・検出速報 2012/13シーズン URL:http://www.nih.go.jp/niid/ja/iasr-inf.html 5)IDWR速報データ2012年第50週 URL:http://www.nih.go.jp/niid/ja/data/3035-idwr-sokuho-data-j-1250.html | |
国立感染症研究所 感染症情報センター/インフルエンザウイルス研究センター | |
2012年12月07日発表
インフルエンザ抗体保有状況
2012年度速報第1号
http://www.nih.go.jp/niid/ja/flu-m/253-idsc/yosoku/sokuhou/2986-flu-yosoku-rapid2012-1.html
| インフルエンザ抗体保有状況 -2012年速報第1報- (2012年12月7日現在) | |
| はじめに 感染症流行予測調査事業における「インフルエンザ感受性調査」は,毎年,インフルエンザの本格的な流行が始まる前に,インフルエンザに対する国民の抗体保有状況(免疫状況)を把握し,抗体保有率が低い年齢層に対するワクチン接種の注意喚起ならびに今後のインフルエンザ対策における資料とすることを目的として実施している。 現在使われているインフルエンザワクチンは,A(H1N1)亜型,A(H3N2)亜型,B型(ビクトリア系統あるいは山形系統)の3つのインフルエンザウイルスがワクチン株として用いられているが,インフルエンザ感受性調査では,これら3つのワクチン株に加え,ワクチンに用いられなかった別系統のB型インフルエンザウイルスについて抗体保有状況の検討を行っている。 本速報では,2012年度の調査によるインフルエンザに対する年齢群別抗体保有状況および前年度調査との比較(第2報以降)について掲載する。 | |
| 1. 調査対象および方法 2012年度の調査は,25都道府県から各198名,合計4,950名を対象として実施された。 インフルエンザウイルスに対する抗体の有無および抗体価の測定は,対象者から採取された血液(血清)を用いて,調査を担当した都道府県衛生研究所において赤血球凝集抑制試験(HI法)により実施された。採血時期は原則として2012年7~9月(例年のインフルエンザの流行シーズン前かつワクチン接種前)とした。また,HI法に用いたインフルエンザウイルス(調査株)は以下の4つであり,このうちa)~c)は2012/13シーズンのインフルエンザワクチンに用いられているウイルス,d)はワクチン株とは異なる系統のB型インフルエンザウイルスであるが,抗体保有状況の把握が必要と考えられるウイルスである。 a) A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型] b) A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型] c) B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)] d) B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)] | |
| 2. 調査結果 2012年12月7日現在,北海道,山形県,福島県,栃木県,千葉県,東京都,神奈川県,新潟県,富山県,石川県,福井県,山梨県,長野県,三重県,山口県,愛媛県,高知県,宮崎県の18都道府県から合計4,955名の対象者についての結果が報告された。5歳ごとの年齢群別対象者数は,0-4歳群:619名,5-9歳群:393名,10-14歳群:409名,15-19歳群:369名,20-24歳群:412名,25-29歳群:445名,30-34歳群:409名,35-39歳群:405名,40-44歳群:371名,45-49歳群:304名,50-54歳群:265名,55-59歳群:212名,60-64歳群:175名,65-69歳群:80名,70歳以上群:87名であった。 なお,本速報における抗体保有率とは,感染リスクを50%に抑える目安と考えられているHI抗体価1:40以上の抗体保有率を示し,抗体保有率が60%以上を「高い」,40%以上60%未満を「比較的高い」,25%以上40%未満を「中程度」,10%以上25%未満を「比較的低い」,5%以上10%未満を「低い」,5%未満を「きわめて低い」と表す。 | |
| 1)年齢群別抗体保有状況 A/California(カリフォルニア)/7/2009 [A(H1N1)pdm09亜型]:図1上段 本ウイルスは2009年に世界的大流行(パンデミック)を起こしたインフルエンザウイルスである。2009/10シーズンは本ウイルスを用いた単価ワクチンが製造され,従来のインフルエンザワクチン(3価ワクチン)とは別に接種が行われたが,2010/11シーズン以降は3シーズン続けてワクチン株の1つとして選定されている。 本ウイルスに対する抗体保有率は,0-4歳群および55歳以上の各年齢群で中程度の抗体保有率(26~36%)であったが,それ以外の年齢群は比較的高い~高い抗体保有率(45~81%)であった。中でも5~24歳の各年齢群は60%以上の抗体保有率(61~81%)であり,15-19歳群で最も高かった。全体の抗体保有率は53.1%であり,調査株中最も高かった。 A/Victoria(ビクトリア)/361/2011 [A(H3N2)亜型]:図1下段 本ウイルスは2012/13シーズンのワクチン株の1つとして選定されたウイルスであり,2010/11~2011/12シーズンにワクチン株であったA/Victoria(ビクトリア)/210/2009から変更となった。 本ウイルスに対する全体の抗体保有率は調査株中2番目に低い42.8%であった。年齢群別では5~44歳の各年齢群および70歳以上群は比較的高い抗体保有率(41~57%)であったが,それ以外の年齢群は中程度以下の抗体保有率(23~36%)であり,特に0-4歳群と65-69歳群は25%未満の抗体保有率(23%)であった。 B/Wisconsin(ウィスコンシン)/1/2010 [B型(山形系統)]:図2上段 本ウイルスは2010年に分離されたB型インフルエンザウイルスであり,2012/13シーズンは4シーズンぶりに山形系統の本ウイルスがワクチン株の1つに選定された。 本ウイルスに対する抗体保有率は,全体では35.0%と調査株中最も低く,年齢群別では20-24歳群をピークに15~34歳の各年齢群のみが40%以上の抗体保有率(42~70%)であった。それ以外の年齢群は中程度以下の抗体保有率(9~39%)を示し,中でも10歳未満および55歳以上の各年齢群は25%未満の抗体保有率(9~24%)であり,65-69歳群で最も低かった。 B/Brisbane(ブリスベン)/60/2008 [B型(ビクトリア系統)]:図2下段 本ウイルスは2009/10~2011/12シーズンまで3シーズン連続してワクチン株に選ばれたウイルスであり,本年度調査におけるビクトリア系統の代表として用いた。 本ウイルスに対する抗体保有率は,0-4歳群および60歳以上の各年齢群で中程度以下の抗体保有率(22~32%)であった。それ以外の年齢群で5~24歳および45~59歳の各年齢群は比較的高い抗体保有率(41~59%)であり,25~44歳の各年齢群は35-39歳群をピークに60%以上の抗体保有率(62~78%)であった。全体の抗体保有率は調査株中2番目に高い52.5%であった。 |
図1
 図2  |
| 2)年齢群別抗体保有状況の前年度調査との比較 ※第2報以降に掲載予定 | |
| コメント 今シーズンは2012年12月7日現在,病原微生物検出情報におけるインフルエンザウイルス分離・検出速報によると,2012年第36~47週(9月3日~11月25日)の期間にA(H1)pdm09亜型が12件,A(H3)亜型が96件,B型が8件(ビクトリア系統:4件,山形系統:1件,系統不明:3件)の報告があり,現時点では主にA(H3)亜型が分離・検出されている1)。また,感染症発生動向調査によるインフルエンザ患者の定点あたり報告数は2012年第47週(11月19日~25日)の速報値で0.22であり2),全国的な流行の指標となる1.0に達していないが,本調査において抗体保有率が低かった年齢層においては,本格的な流行シーズンが始まる前にワクチン接種等の予防対策を行うことが望まれる。 | |
| 1)病原微生物検出情報‐インフルエンザウイルス分離・検出速報 2012/13シーズン 国立感染症研究所HP [http://www.nih.go.jp/niid/ja/iasr-inf.html] 2)感染症発生動向調査‐速報データ2012年第47週 国立感染症研究所HP [http://www.nih.go.jp/niid/ja/data/2958-idwr-sokuho-data-j-1247.html] | |
国立感染症研究所 感染症情報センター/インフルエンザウイルス研究センター | |
日本の2013年までの各週のインフルエンザ(風邪)ビールスの、インフルエンザb、インフルエンザA(H3)、インフルエンザA(H1)、インフルエンザA(H1)pdm09の 発生数、発生割合
https://nesid3g.mhlw.go.jp/Byogentai/Pdf/data2j.pdf

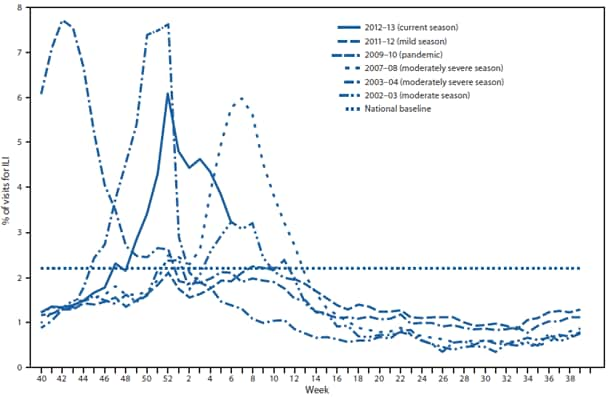
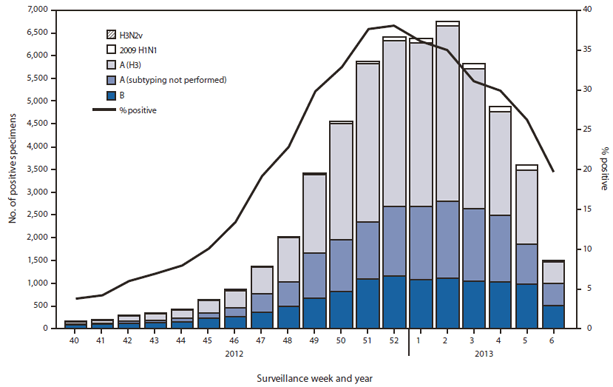 Alternate Text: The figure above shows the number and percentage of respiratory specimens testing positive for influenza, by type, surveillance week, and year in the United States, during the 2012-13 influenza season, according to U.S. World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories. During September 30, 2012-February 9, 2013, approxi¬mately 140 WHO and NREVSS collaborat¬ing laboratories in the U.S. tested 203,706 respiratory specimens for influenza viruses; 55,470 (27.2%) were positive.
Alternate Text: The figure above shows the number and percentage of respiratory specimens testing positive for influenza, by type, surveillance week, and year in the United States, during the 2012-13 influenza season, according to U.S. World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories. During September 30, 2012-February 9, 2013, approxi¬mately 140 WHO and NREVSS collaborat¬ing laboratories in the U.S. tested 203,706 respiratory specimens for influenza viruses; 55,470 (27.2%) were positive.